Temple Hair Loss: Causes, Prevention, and Treatment Options
Written by
Megan Brooks
Last modified
SHARE ON
Table of Contents
Contact our specialists now for Hair Replacement!
Share this article
Introduction
Temple hair loss is when hair thins or falls out around your temples(the parts above your ears extending toward your forehead). If you see your hairline moving back, scalp showing, or patches starting near the temples, you’re not alone.
Many people ignore these early signs.
In this blog, you will learn what temple hair loss is, how it shows in men and women, why it happens, what you can do now to stop it, and how non-surgical solutions (like hair systems or wigs) can give you confidence while natural regrowth works.
Key takeaways
Temple hair loss begins with subtle signs like finer hair, scalp visibility, and uneven thinning — recognising it early improves recovery chances.
Causes range from androgenetic and traction alopecia to hormonal shifts, nutrient deficiencies, and scarring disorders — diagnosis is key.
Men usually show sharp temple recession, while women experience diffuse thinning linked to hormonal and stress-related changes.
Effective treatments include minoxidil, PRP therapy, oral medications, and customised non-surgical hair loss solutions like hair systems/wigs.
Long-term prevention requires gentle styling, scalp care, balanced nutrition, and early consultation with a trichologist to protect active follicles.
What Is Temple Hair Loss?
Temple hair loss refers to the gradual thinning and recession of hair specifically at the temporal regions of your scalp, those areas on either side of your forehead, just above your ears. It’s where your hairline meets your forehead at the sides.
This can happen gradually or more suddenly. The causes vary. Some are temporary; others are permanent if not addressed early.
Men vs Women
Women and men can both get temple hair thinning, but the patterns differ. Below is a simple table comparing:
Feature
Men
Women
Common pattern
Receding hairline at temples, changing “M” shape.
More diffuse thinning, sometimes slight temple recession.
Role of hormones
Strong link to DHT, androgen sensitivity.
Hormonal fluctuations (menopause, PCOS) can lead to a lower DHT effect.
Speed
Often faster once started.
Usually slower, it may remain mild for a long time.
Likelihood of transplant or permanent loss
Higher if late stage.
More risk of diffuse thinning, less dramatic temple recession.
Symptoms Of Temple Hair Loss
Here is what most articles won’t tell you: the symptoms go far beyond just seeing less hair.
1. Physical Symptoms You Can See and Feel
Hairline recession: Your temples are moving backwards, creating a deeper "M" shape or widening the gap between your forehead and where your hair begins.
Increased scalp visibility: You can see more skin through your hair at the temples, especially in bright lighting or photographs.
Hair texture changes: The hair at your temples feels finer, softer, and more fragile than the hair elsewhere on your head.
Miniaturisation: Short, thin, almost transparent hairs appear where thick terminal hairs once grew; these are follicles in their death throes.
Asymmetrical thinning: One temple often recedes faster than the other, creating an unbalanced appearance.
2. The Early Warnings Most People Miss:
Excessive shedding during washing: You notice significantly more hair coming away when you wash or condition your hair, particularly from the temple area.
Hair takes longer to grow: Hair at your temples seems to grow more slowly or not at all, whilst the rest of your hair continues at a normal pace.
Increased hair on your pillow: You wake to find more hair on your pillowcase, concentrated from the sides of your head.
Changes in your hairline shadow: When you look closely in natural light, you see a "shadow" of fine, colourless vellus hairs where thick pigmented hair once was.
Wider forehead appearance: Your forehead looks larger, particularly in photos, even if you haven't consciously noticed hairline changes.
Itching or tingling: Some people experience mild scalp irritation, tightness, or tingling at the temples before visible thinning occurs; this is follicular inflammation.
3. Physical Sensations That Indicate Follicle Distress
Scalp sensitivity: The skin at your temples feels more tender or sensitive to touch.
Tightness: A sensation of tightness across the temporal regions, often described as a "band-like" feeling.
Burning or stinging: Mild discomfort that comes and goes, particularly after hair washing or styling.
Oilier or drier scalp: Changes in sebum production at the temples specifically.
4. Psychological and Emotional Symptoms
This is where competitors’ articles fall short. They don’t acknowledge that hair loss on the temples affects your mental well-being, often before it becomes visibly obvious to others.
Increased self-consciousness: You find yourself constantly touching your temples, checking mirrors, or taking photos to compare your hairline.
Styling anxiety: You spend more time arranging your hair to conceal thinning, perhaps changing your parting or fringe.
Avoidance behaviours: You avoid bright lighting, being photographed from certain angles, or activities that might reveal your hairline (swimming, wind, rain).
Social withdrawal: Some people begin avoiding social situations because they feel self-conscious about their appearance.
Reduced confidence: Particularly in professional or romantic contexts where first impressions feel crucial.
Anticipatory grief: A sense of loss for how you used to look, and anxiety about how much worse it might become.
| Understanding the timeline helps you gauge where you are in the process:
Stage 1 (Subtle changes, Age 18-30 typically)
Stage 2 (Noticeable recession, Age 25-35 typically)
Stage 3 (Significant recession, Age 30-40 typically)
The most common cause. In men, DHT (a hormone) shrinks follicles in sensitive areas like the temples. Over time, they produce thinner hair, then no hair.
In women, it causes diffuse thinning; temple recession is less sharp but possible.
2. Traction Alopecia
Caused by repeated tension (tight ponytails, braids, extensions). The temples are vulnerable. If caught early, damage may be reversible.
Note – Traction alopecia commonly occurs in Afro-Caribbean hairstyles that involve tight braids. Hair loss typically begins in childhood and may initially be reversible. The condition follows a biphasic pattern, with early-stage disease being nonscarring and reversible, while chronic cases result in permanent scarring alopecia.
3. Telogen Effluvium
A shock (stress, surgery, illness, crash diet) pushes many hair follicles into the resting phase.
You’ll see shedding across the scalp, but temples often show earlier because hair is already less dense there.
4. Scarring / Cicatricial Alopecias
Conditions like frontal fibrosing alopecia (especially in post-menopausal women) damage hair follicles irreversibly, replacing them with scar tissue.
Also, lichen planopilaris, central centrifugal cicatricial alopecia may affect edges.
Low iron, zinc, protein deficiency, vitamin D, and B vitamins — these weaken follicles.
Also, reduced blood flow or microvascular issues in the temple region may exacerbate the issue (a few articles mention that, so this is a gap to emphasise).
9. Autoimmune Alopecia
Alopecia areata can cause patchy hair loss that may include the temples.
10. Medication / Drugs / Systemic Illness
Some medications (anti-inflammatories, hormones, chemotherapy) cause hair loss, including temples.
Temple Hair Loss in Men vs. Women
Aspect
Men
Women
Primary cause
Androgenetic alopecia (male pattern baldness) is driven by genetic DHT sensitivity.
Hair becomes finer and less dense but may retain some pigmentation longer; women often retain more vellus hairs.
Genetic disposition
Strong genetic component; 80% predictable from family history; both maternal and paternal genes involved.
Genetic factors present but less predictable; multiple genes involved; family history less reliable predictor.
Hormonal factors
Primarily DHT sensitivity; testosterone levels may be normal but conversion to DHT is key; it rarely involves thyroid or other hormones.
Complex hormonal interactions: oestrogen, progesterone, androgens, thyroid hormones, prolactin; PCOS, menopause, and pregnancy are all significant.
Associated conditions
Generally occurs as an isolated condition; cardiovascular risk may be elevated in early-onset cases.
Often accompanied by other hormonal symptoms: menstrual irregularities, PCOS, thyroid disorders, and iron deficiency anaemia.
Traction alopecia risk
Lower risk primarily affects those with tight hairstyles, man buns, cornrows, or sports helmets.
Much higher risk; years of ponytails, braids, hair extensions, and tight updos contribute significantly to temple thinning.
Psychological impact
Significant but somewhat normalised socially, it still affects self-esteem, perceived attractiveness, and confidence.
Profoundly distressing; female hair loss is less socially accepted; greater impact on self-identity and emotional well-being.
Styling adaptations
Shorter styles often work better; some embrace the bald look; less pressure to conceal thinning.
More styling pressure, longer hair to camouflage, fringe adjustments, toppers and extensions are more commonly used.
Treatment urgency
Moderate urgency; earlier treatment is more effective, but progression is predictable.
Higher urgency for diagnosis; distinguishing the cause is critical; some causes (FFA) require prompt treatment to prevent permanent loss.
Nutritional factors
Less commonly causative unless severely deficient, iron deficiency is rare in men.
Frequently contributory; iron deficiency is extremely common in menstruating women; dietary restrictions and dieting play a larger role.
Stress-related loss
Less common as a primary cause; may accelerate existing androgenetic alopecia.
More susceptible to telogen effluvium from stress, illness, and childbirth; temples are often the first visible area affected.
Women shouldn’t assume their temple thinning is the same as male pattern baldness, and men shouldn’t overlook potential underlying health conditions. Both benefit from proper diagnosis before rushing into treatment.
Effective Treatments for Temple Hair Loss
Here you will find the solutions that work:
Minoxidil (Rogaine):
A topical solution or water-based formulation applied directly to the scalp. It’s available over-the-counter in 2% and 5% concentrations.
Finasteride (Propecia, Proscar):
An oral medication taken daily, available by prescription. The standard dose for hair loss is 1mg daily.
Dutasteride:
Similar to finasteride but more potent. It blocks both Type I and Type II 5-alpha-reductase enzymes, reducing DHT by approximately 90% (compared to finasteride’s 70%).
Spironolactone (Women):
An oral medication that blocks androgen receptors and reduces testosterone production. Originally a blood pressure medication.
Oral Minoxidil :
Taking minoxidil as a tablet rather than applying it topically. Doses for hair loss are very low (0.25-5mg daily) compared to the high doses used for blood pressure.
Platelet-Rich Plasma (PRP) Therapy:
A procedure where your blood is drawn, processed to concentrate platelets, and then injected into your scalp. Platelets contain growth factors that may stimulate follicles.
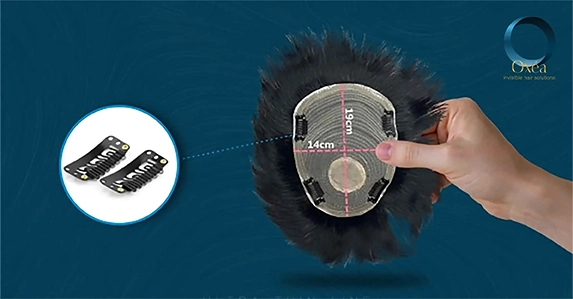
Hair Systems / Customised Wigs :
A well-fitted hair system can cover thinning temples instantly. It is non-invasive, customizable (colour, density, texture), and allows you to look good while healing or regrowth happens. It’s a valid temple hair loss solution.
Low-Level Laser Therapy (LLLT):
Medical devices (combs, caps, helmets) that emit specific wavelengths of red light onto the scalp.
Scalp Micropigmentation (SMP) :
Tiny pigment dots create the illusion of follicle density near temples. Good for mild recession or to complement hair systems.
Shedding is temporary hair fall where follicles remain healthy and regrowth returns. Hair thinning is a progressive reduction in hair density caused by follicle miniaturisation; new growth gets finer with each cycle. Shedding often resolves itself; thinning typically requires intervention.
Yes. Stress typically triggers shedding (telogen effluvium) first. If chronic, it can contribute to hormonal changes that accelerate follicle miniaturisation, particularly in those already genetically predisposed to pattern hair loss.
Check the root of fallen hairs for a white bulb (healthy shed). Compare the parting width photos over four weeks. Assess whether the new regrowth is as thick as your established hair. If density is progressively reducing, thinning is more likely than temporary shedding.
Shedding-related thinning often is, once the trigger is resolved. Genetic or follicle miniaturisation-based thinning is not easily reversed, but it can be slowed or addressed immediately with a non-surgical hair replacement system that delivers natural results from day one.
Whether you’re dealing with early thinning or advanced recession, whether you’re a man in your twenties or a woman going through menopause, there are proven, effective options available to you right now.
Start with understanding. Know what type of hair loss at temples you’re experiencing. Get a proper diagnosis. Address underlying health issues. Then, choose your path forward.
If you want immediate results and confidence whilst pursuing long-term treatments, Oxea London’s hair systems offer natural-looking solutions that let you live your life fully whilst your treatments work.
Author Profile
Megan Brooks
Megan Brooks is a Certified Trichologist at Oxea Invisible Hair Solutions with over 21 years of Unbeatable experience. Throughout her remarkable career, she has successfully completed an impressive 8000+ hair replacement systems. Megan is dedicated to transforming lives and boosting self-confidence so that one can live with all the pride. She has served over 800 satisfied clients and still-counting, while helping them regain their natural appearance and feel their best.